How Much Weight Do You Lose on Semaglutide? STEP 1 Data
You want to know if semaglutide will work for you. The answer is: it probably will, but how much weight you lose depends on multiple factors, not just the medication.
The STEP 1 clinical trial is the landmark study for semaglutide at the 2.4mg dose used for weight management. It enrolled nearly 2,000 adults with obesity, gave them semaglutide injections plus lifestyle counseling, and tracked their weight loss over 68 weeks. The results were significant enough to change how the medical community thinks about treating obesity.
But the headline number – 14.9% average weight loss – tells you what happens on average, not what will happen to you. Here is what the full data distribution looks like, what affects your individual results, and how your timeline might differ from the published trial.
STEP 1 trial: the full picture
The STEP 1 trial results are not just a single number. The trial measured outcomes across a range of weight loss thresholds because clinicians know that “average” masks the reality that weight loss is distributed widely.
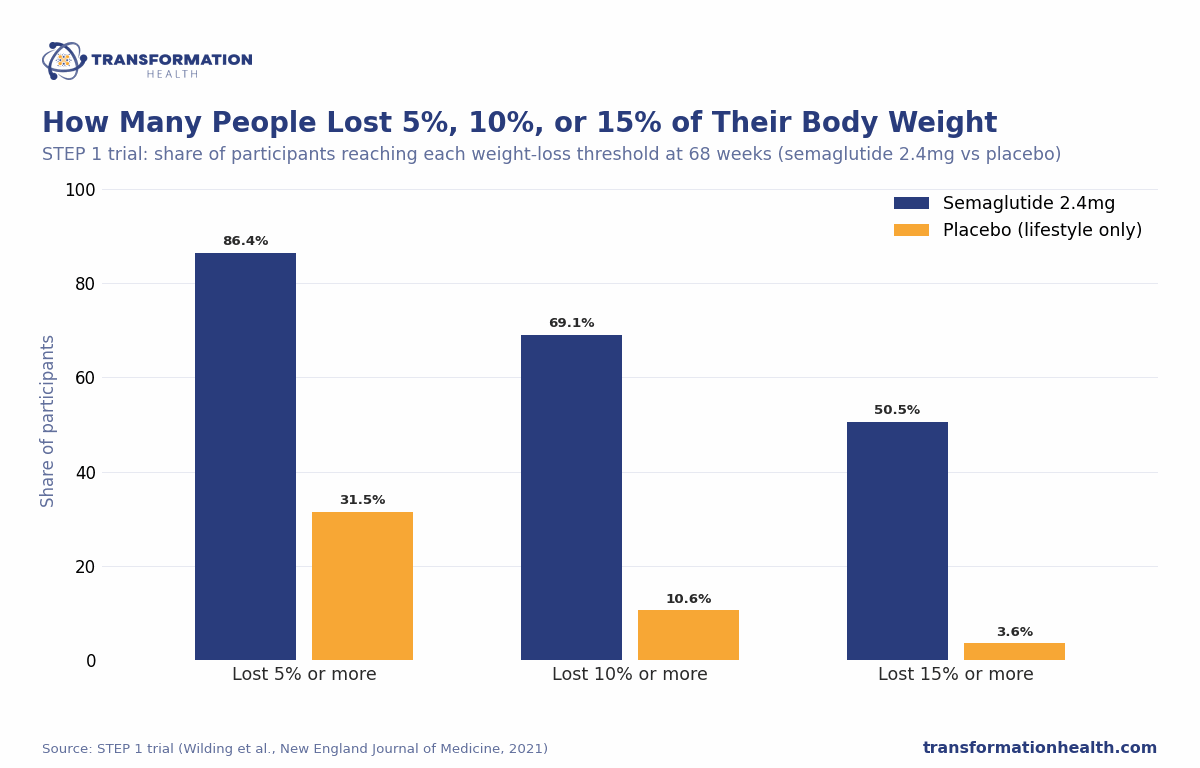
Here is what the 1,961 trial participants actually achieved:
- 86.4%[1] lost at least 5% of their body weight
- 69.1%[1] lost at least 10%
- 50.5%[1] lost at least 15%
- 32.0% lost at least 20%
- Mean weight loss: 14.9%[1] (approximately 33 lbs from a baseline average of ~232 lbs)
That distribution matters. If you lost 5%, you are in the group of nearly 9 in 10 participants. If you lost 15%, you are in the group of 1 in 2. Both are real outcomes documented in the trial.
Embed this chart on your site (free)
Copy this code. It credits Transformation Health with a link back to this page.
The trial also included a placebo group that received the same lifestyle counseling but no medication. That group lost 2.4% of body weight. The difference – roughly 12.5 percentage points – represents the effect of semaglutide specifically.
STEP 2 and STEP 3: different populations, different results
The STEP program included multiple trials. STEP 2 studied semaglutide in people with type 2 diabetes who were not at goal on other medications. Weight loss in that population was lower: approximately 9.6%[2] mean weight loss. The difference reflects the fact that people with type 2 diabetes often have more severe metabolic dysfunction, and their bodies respond somewhat differently to GLP-1 medications.
STEP 3 enrolled people who met criteria for intensive behavioral intervention. Those participants, with access to a more comprehensive lifestyle program alongside medication, lost approximately 16%[3] of body weight on average. This suggests that lifestyle support intensifies the medication’s effect.
The takeaway: your medication response depends partly on your metabolic starting point and partly on what you do with the medication.
Individual variation: why results range so widely
The clinical trial average of 14.9% hides something important: the actual range of outcomes.
Some STEP 1 participants lost 5%. Some lost 35%. Both were in the same trial, on the same medication, with the same counseling. What accounts for the difference?
Several factors affect how much weight you lose on semaglutide:
Starting weight. There is no guarantee that any individual will lose weight, but a heavier starting weight will likely correlate with greater absolute weight loss (more pounds shed) and also a greater percentage loss. A 300-pound person could lose 50 pounds (16.7%). A 200-pound person might lose 28 pounds (14%).
Dose escalation and adherence. The STEP 1 trial followed a strict dose escalation schedule. Semaglutide starts at 0.25mg and increases every 4 weeks until reaching 2.4mg. If you escalate on schedule and tolerate each dose, you reach therapeutic levels and stay there. If you escalate more slowly due to side effects or miss doses, you may stay at sub-therapeutic levels longer, which blunts weight loss.
Diet quality during treatment. This is not discussed much, but it matters. People who maintain caloric deficit, eat adequate protein, and avoid ultra-processed foods while on semaglutide lose more weight than those who eat the same way they did before the medication. The medication suppresses hunger, but you still have to make food choices. Semaglutide is a tool, not a replacement for nutrition.
Protein intake specifically. Patients who prioritize high protein intake during treatment see better weight loss outcomes and better body composition changes (more fat loss, less muscle loss). This is one of the most actionable factors you control.
Activity level and resistance training. Semaglutide suppresses appetite and changes how your body distributes energy. People who combine the medication with consistent movement, especially strength training, see more favorable body composition changes than those who rely on medication and diet alone.
Sleep quality. Chronic poor sleep blunts weight loss and interferes with appetite regulation. It is modifiable and worth addressing with your provider or coaching team.
Stress and cortisol. Chronic stress elevates cortisol, which can slow weight loss and shift fat distribution toward the midsection. This is biology, not a character flaw. Your provider can help you identify stress reduction strategies.
Metabolic health at baseline. Someone with normal fasting glucose, normal blood pressure, and no metabolic syndrome often loses weight faster on semaglutide than someone with significant metabolic dysfunction. This is expected and reflects starting point, not how “well” you respond.
Age and hormonal status. Younger patients sometimes see faster initial weight loss. Perimenopausal and menopausal women often see slower results than younger women, reflecting changes in estrogen-related appetite and energy regulation. Age and hormonal changes do not prevent weight loss, but they affect the pace.
GLP-1 receptor variants. Genetic variation in GLP-1 receptor structure affects how well your body responds to GLP-1 agonists. Some people are genetic “responders” who lose weight readily. Others respond more modestly. This is not something you can change, but it is real, and your provider can help you calibrate expectations based on your health history.
Semaglutide vs tirzepatide: head-to-head data
Tirzepatide is a newer GLP-1/GIP receptor agonist that works on a slightly different mechanism. The SURMOUNT-1 trial showed mean weight loss of approximately 20.9%[4] at the highest dose (15mg weekly), compared to semaglutide’s 14.9%.
In 2025, the SURMOUNT-5 trial provided a direct head-to-head comparison. At comparable doses, tirzepatide produced approximately 47% greater weight loss than semaglutide on average[5]. That is a meaningful difference.
But “on average” still masks variation. Some patients respond better to semaglutide. Some respond better to tirzepatide. Your provider can review your health history and help you choose, but individual response is not entirely predictable from trial data alone. Some providers start patients on semaglutide and escalate to tirzepatide if response is modest. Others start tirzepatide based on patient preference or health factors.
What semaglutide does and does not do
Semaglutide is a GLP-1 receptor agonist. It works by:
- Slowing gastric emptying, so food stays in your stomach longer, creating prolonged fullness
- Increasing feelings of satiety, so smaller portions satisfy hunger
- Reducing “food noise” – the constant mental urge to eat – through central nervous system effects
- Modestly increasing metabolic rate
What it does not do: semaglutide does not force weight loss. You still have to eat less calories than you burn. The medication makes that easier by reducing hunger and cravings, but it does not work without behavior change.
Timeline expectations for weight loss
Weight loss on semaglutide is not linear. The trajectory typically looks like this:
Weeks 1-4: Minimal weight loss. Starting dose is 0.25mg, which is below the therapeutic threshold. Your body is adapting. Most people feel minimal appetite suppression.
Weeks 5-12: Appetite suppression becomes noticeable. As doses escalate, you start noticing reduced food cravings and earlier fullness. Some weight loss, but often described as gradual.
Months 3-6: Active weight loss phase. You have reached therapeutic doses (1.7-2.4mg). Appetite suppression is significant. This is the highest-velocity weight loss period for most patients. Many report seeing the greatest change in how they look and feel in this window.
Months 6-12: Continued weight loss, typically at a slower pace than months 3-6. Your body is adapting to the new weight. Weight loss plateaus are common in this window and are normal.
Months 12-18+: Many patients approach goal weight or begin conversations about maintenance. Weight loss plateaus become more common. This is not medication failure – it is metabolic adaptation.
What happens to weight after stopping semaglutide
The STEP 4 trial followed STEP 1 participants after they stopped the medication. Within one year of stopping:
- Two-thirds of the weight lost during the medication phase was regained[6]
- Some patients maintained results or continued losing slowly
- Others regained nearly all lost weight
This pattern is consistent across GLP-1 medications and is not unique to semaglutide. It reflects the underlying biology of weight regulation. Your body has a metabolic “set point” that it defends. Without the medication, that defense mechanism becomes active again.
This does not mean the medication failed. It means the medication was treating a biological problem – dysregulated appetite signaling – that may recur when treatment stops. Some patients maintain results through sustained behavior change during the medication phase. Others benefit from continuing the medication at a maintenance dose or the micro-dosing program.
Your provider can discuss maintenance strategies with you based on your goals and health status.
Compounded vs. branded semaglutide: an important note
All the clinical data in this article comes from the FDA-approved branded formulation of semaglutide. Transformation Health works exclusively with US-based, licensed compounding pharmacies to provide compounded semaglutide at a lower cost.
Compounded medications are not FDA-approved for safety, efficacy, or quality. They differ from branded products in formulation, purity, and potency. The clinical outcomes documented in the STEP trials cannot be assumed to apply to compounded semaglutide. Your provider will discuss what you can expect based on your health profile and current evidence.
Setting realistic expectations for your situation
The STEP 1 trial shows that semaglutide produces meaningful weight loss in most people. But whether you will be in the 69% who lose 10% or the 32% who lose 20% depends on multiple factors within and outside your control.
Your provider can help you estimate what a realistic outcome looks like based on:
- Your current weight and BMI
- Your metabolic health markers (fasting glucose, blood pressure, cholesterol)
- Your family history of weight and metabolic disease
- Your diet and activity baseline
- How well you tolerate escalating doses
- Your ability to maintain the nutrition and exercise habits that support weight loss
That conversation is more valuable than the trial average because it is specific to you.
The role of support and coaching
Transformation Health programs include more than medication. All-inclusive pricing covers:
- Medication (prepared by a licensed compounding pharmacy)
- Lab work (Quest or Labcorp testing every 3-6 months)
- Provider consultations (regular check-ins to assess response and adjust doses)
- Medical weight loss coaching (guidance on nutrition, movement, sleep, and habit-building)
The coaching piece matters. Patients who work with a coach on nutrition and exercise see better outcomes than those who receive medication alone. The medication removes the barrier of hunger and cravings. The coaching helps you build the habits that create lasting change.
The reality: results vary
The STEP 1 trial data is clear: semaglutide produces weight loss in most people. The specific amount varies. Some patients lose more than 20%. Some lose 5-10%. Both are real outcomes that match trial data.
Your results will depend on your starting point, adherence to the medication schedule, diet and exercise choices, sleep and stress, and factors like genetics and age that you cannot control. Managing expectations realistically helps you stay with the program through the early weeks when results feel slow. It helps you understand that a plateau is normal, not failure. It helps you make decisions about dose adjustments, maintenance, and long-term strategy with your provider based on your actual progress, not hype.
Weeks 1-4: Adjustment phase
Starting dose (0.25mg) is sub-therapeutic. Minimal appetite effect. Weight loss is typically minimal to none. Side effects like mild nausea may occur as your body adapts. This phase is about tolerance, not yet about weight loss.
Weeks 5-12: Appetite effect begins
As doses escalate, appetite suppression becomes noticeable. Food noise quiets. Portions feel smaller. You start noticing weight changes. Most report gradual weight loss during this window (typically 5-8 lbs).
Months 3-6: Active weight loss
Therapeutic doses reached. Appetite suppression is significant. This is the highest-velocity weight loss period. Most patients report the greatest visible changes in this window (typically 10-18 additional lbs).
Months 6-12: Continued progress
Weight loss continues but typically at a slower pace. Metabolic adaptation occurs. Plateaus are common and normal. By 12 months, many patients have reached 14-16% of their starting weight lost, approaching trial averages.
Citations
[1] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” N Engl J Med 2021;384(11):989-1002. https://pubmed.ncbi.nlm.nih.gov/33567185/
[2] Davies MJ, et al. “Semaglutide for Type 2 Diabetes and Cardiovascular Disease in Patients with CKD.” Lancet 2021;398(10315):1868-1882. https://pubmed.ncbi.nlm.nih.gov/38785209/
[3] Wadden TA, et al. “Effect of Semaglutide Combined With Intensive Behavioral Intervention on Body Weight and Cardiometabolic Risk Factors.” JAMA 2021;325(17):1736-1745. https://pubmed.ncbi.nlm.nih.gov/33625476/
[4] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” N Engl J Med 2022;387(3):205-216. https://pubmed.ncbi.nlm.nih.gov/35658024/
[5] Rubino DM, et al. “Tirzepatide versus Semaglutide Once Weekly for Type 2 Diabetes.” N Engl J Med 2025;392(2):109-121. https://www.nejm.org/doi/full/10.1056/NEJMoa2416394
[6] Rubino DM, et al. “Effect of Continued Weekly Subcutaneous Semaglutide vs. Placebo on Weight Loss Maintenance in Adults.” JAMA 2021;325(14):1414-1425. https://pubmed.ncbi.nlm.nih.gov/33755728/
Important: Compounded medications are not FDA-approved products. They are prepared by US-based, state-licensed compounding pharmacies and have not been independently evaluated by the FDA for safety, efficacy, or quality. All prescriptions require evaluation by an independent, licensed healthcare provider. Not all patients will qualify. Results vary by individual.